
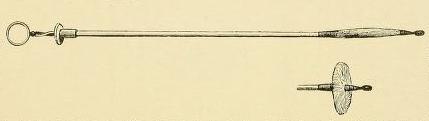
Graefe Coin-Catcher (Münzenfänger), 1850-1900. 42 cm, metal working part 1, 5 x 1, 2 cm. NML Medical Museum Instrument Collection, N 354. Photography by Veronika Löblová
Object of the Month: February 2020
Coin-Catcher
How best to remove a five franc coin stuck in the pharynx or the esophagus?
Until the early 20 century, foreign objects were often removed from the throat without eye control. Instruments for such operations were often introduced centuries ago. “Coin catcher” after C. F. Graefe, an instrument in the shape of a metal umbrella used to draw larger, flat objects from the gullet, became very popular during the 19 century. A double metal leaf on the end of an elastic whalebone stick should easily grasp a coin or a button and bring it back through the mouth. Before endoscopic instruments for the esophagus (esophagoscopes) were introduced, such operation was necessary to remove objects that could not be vomited out. The risks of damage to the esophagus wall and resulting infection were, however, dire. Specialists rejected such instruments since the late 1800s, yet the “old instrumentarium” took decades to disappear from medical practice.
Physicians and surgeons have employed instruments to pull foreign bodies from the gullet for centuries. For removing bones, coins or needles, a sponge or a hairball tied to a thread were used, as were long forceps and hooks: a flexible probe, a thin wax candle or a leek stalk pushed an object down to the stomach. The German surgeon, alchemist and botanist Hieronymus Brunschwig (ca. 1450-1512) described a „lead hammer“ (Bleihammer), a small lead sphere on a twine that descends into the esophagus by its own weight, can be pulled out repeatedly and jerks the swallowed object loose. The probang (Schlundstösser), a perforated staff ending in a lump of sponge, was widespread during the Renaissance. Sharp needles or small bones were caught in the holes on the stick, made of metal wire or later – since Thomas Willis (1621-1675) of softer and more elastic whalebone. The sponge needed to pass easily through the esophagus and around the blockage and yet envelop the foreign body: the surgeon of the Dauphin, Prudent Hévin (1715-1789) bound it with a piece of chamois, wound around with double thread. Withdrawing the thread pulls the leather out or apart and the sponge returns to its former shape and size.
Surgeons of the 18 and 19 centuries introduced a number of instruments for extraction of foreign bodies from both the gastrointestinal and the respiratory tracts, including different types of esophagus forceps. Many of the innovations were described and even designed by the surgeon of the St. James Hospital and the Professor of the Leipzig University, Johann Gottlob Eckoldt (1746-1809), the author of a comprehensive tract on the subject. The „grate catcher“ (Grätenfänger), named after its alleged inventor, the Scottish surgeon Sir William Fergusson (1808-1870), and its first producer, the London instrument maker John Weiss (1773-1843), became popular for the removal of sharp, small objects, such as needles or fish bones. A sheaf of horse hair was enveloped with a leather or rubber pipe and a sphere of sponge or fabric was attached at the end. A shaft of whalebone passed in the middle of the sheaf. Pulling the shaft out opened a wide circular fan of hairs that sweepes up small fragments and constricted again before it is withdrawn. In the Czech medical journal, Časopis lékařů českých, the city physician in Příbram Karel Kavalier (Kavalír, 1835-1897) gave his experience with the instrument in 1867.
{kind=link}
Friedrich von Esmarch, Ernst Kowalzik, Chirurgische Technik, 3, Operationen am Kopf und Hals (Kiel und Leipzig: Lipsius und Tischer, 1899), 219.
An instrument in the shape of a metal „umbrella“ was used for removal of larger, flat objects. The „coin catcher“ (Münzenfänger), also known as „Gräfe‘s basket“ or „money probang“ in English, became the instrument of choice for such operations during the 19 century. It carried the name of the Berlin surgeon Carl Ferdinand von Gräfe (1787-1840). At the end of a whalebone stick, a double metal plate, perforated on each side, or a double loop is attached on a hinge. Before the operation, the patient should drink oil or egg whites to ease the slide of the basket into the gullet. The surgeon pushes down the tongue and presses the plate against the side of the pharynx, the staff bends and the oiled instrument slides down. When the blocking object is located, the end of the staff is forced against the esophagus wall, the basket tilts and engages the object. A reverse pull on the handle pulls the instrument out with the foreign body. If the instrument be stuck, the surgeon turns it to the side, disengages it and repeats the operation after a while.
An engraving of a similar tool was published by Eckoldt (1799). He claims it is “more suitable than wire hooks for the removal of coins, buttons, and other flat bodies …. [but] who invented it, remains unknown to me.” The instrument has a flexible whalebone handle and the round, blunt end protects the esophagus wall. “I have seen these instruments used to much success in London children, where a widespread game involves casting a coin into the air and catching it by mouth, giving one a bigger chance of swallowing a coin than is the case elsewhere.” Franz Andreas Ott presented it as an improvement from Savigny’s hook on a leather-coated whalebone stick.
In France, the „coin catcher“ gained currency after May 14, 1830, when Guillaume Dupuytren (1777-1835) used it in the Hôtel-Dieu hospital to remove a five franc coin from the lower pharynx of a twenty-five year old man. Previous attempts with a variety of pincers and forceps had been fruitless. The reports do not say how did the youth swallow the coin: during the 19 century, many other case histories list a five-franc piece. To swallow a coin with the likeness of the King, the diameter of 37 millimeters and the weight of 25 grams, clearly carried its risks.
{kind=link}
The same was, however, the case regarding the instrument. César-Alphonse Robert (1801-1862) began using it not only for coins, but also bone fragments and other voluminous bodies. In the 1867 volume of the journal Vierteljahrschrift für die praktische Heilkunde, published in Prague since 1844, Georg von Adelmann (1811-1888), Professor of Surgery in Tartu (Dorpat), described 11 cases of coin removal using the coin catcher (of a total of 33) and also 3 successful operations of swallowed bone. Adelmann himself was not so successful, as an 1857 case history, described here in some detail, shows. A 39 year old peasant purchased a piece of lamb meat with bone on the market. When eating, he was distracted and swallowed a two-inch bone by accident. The fragment lodged under the cricoid cartilage (between the pharynx and the esophagus) and all effort to swallow only moved it deeper. Adelmann failed to grasp it with forceps (after Eckoldt) and forcing it down using probang, did not reach the stomach by any means. He succeeded, after several attempts, to squeeze the metal basket alongside the bone, but the latter did not move and the catcher itself became stuck. On the third day, the surgeon managed to liberate the tool with a rubber tube, having administered belladonna as an anesthetic and to suppress the emetic reflex. Subsequently, he tried to push the fragment into the stomach with a probe. This seemed to work and the patient was released. A week later, however, he brought the bone he threw up in the meantime to the clinic and on the following day, he died from esophagus perforation and the resulting respiratory infection.
The Parisian instrument maker Joseph Charriere (1803-1876) placed a piece of sponge (a probang) on the opposite end of the staff, to enable using the instrument both for pulling out and for pushing in. Similar instrument combination have been common in the 19 and 20 centuries: the price of expanding sets of specialized instruments may be among the reasons.

Friedrich von Esmarch, Ernst Kowalzik, Chirurgische Technik, 3, Operationen am Kopf und Hals (Kiel und Leipzig: Lipsius und Tischer, 1899), 219.
The Gräfe coin catcher remained popular until the late 19 century. With the advancement of esophagoscopy since the 1880s, doubts about the „old instrumentarium“ grew. The risks of damaging the esophagus wall became untenable when the course of the operation can be followed visually. The use of the catcher or probang was made no safer when checked by the X-Ray and the long-term X-Ray exposure caused further harm. At the same time, asepsis became the standard in surgery and the advantages of whalebone, both firm and elastic, paled when the instrument could not be sterilized.

Short esophagoscope with distal lighting for examination of the region connecting the pharynx and the esophagus. Pilling (Philadelphia), 1920s- 1930s. NML Medical Museum, P 996. Photograph by Veronika Löblová
Nonetheless, we find this instrument both in the 1905 Waldek and Wagner (Prague) and in the 1920s Aesculap (Jetter und Scheerer, Tübingen) catalogues. The otorhinolaryngologist Václav Tesař (1890-1967) issued a stern warning against the „old dangerous instruments“ in 1934, one repeated by Michal Sivák (1899-1966) as late as 1943. Such devices appear to have remained popular – among GPs in particular – at least during the war.
Today, we would hardly find a doctor or a patient that has seen them used. Or are we wrong and someone among our readers remembers seeing them or being told of them?